Understanding Defibrillation Waveforms
Let’s define a few terms:
Energy: Energy in a defibrillator is expressed in joules. A joule is the unit of work associated with one amp of current passed through one ohm of resistance for one second.
When we express it in a formula, it is generally stated as follows:
- Joules (Energy) = Voltage X Current X Time
- Joules have become a surrogate for current in modern defibrillator language.
Current: Current is what actually defibrillates the heart. It is also expressed as Voltage/Impedance (resistance).
Impedance: Resistance to Flow; there is resistance in the electrical circuit itself as well as in the patient. The amount of impedance in a patient is difficult to determine as it relates to body mass, temperature, diaphoresis, and quality of the contact with paddles or pads. Impedance is expressed in ohms.
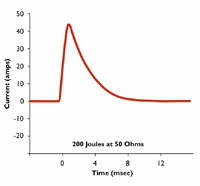
Monophasic Waveforms: A type of defibrillation waveform in which a shock is delivered to the heart from one vector as shown below. It is shown graphically as current vs. time.
In this waveform, there is no ability to adjust for patient impedance, and it is generally recommended that all monophasic defibrillators deliver 360J of energy in adult patients to insure maximum current is delivered when patient impedance can not be detected.

Biphasic Waveforms: A type of defibrillation waveform where a shock is delivered to the heart via two vectors. Biphasic waveforms were initially developed for use in implantable defibrillators and have since become the standard in external defibrillators.
While all biphasic waveforms have been shown to allow termination of VF at lower current than monophasic defibrillators, there are two types of waveforms used in external defibrillators. These are shown below.

Defibrillator manufacturers have approached biphasic defibrillation differently.

Both Physio-Control and Philips use the biphasic truncated exponential (BTE) waveform originally developed for internal defibrillators, though they use different energy settings with the waveform. Physio-Control uses what is termed a “high energy” biphasic waveform, which is also known as ADAPTIV™ Biphasic. Physio-Control energy settings go up to 360 joules of energy and they essentially distribute the voltage and current available over a wider range of energy settings. Additionally, they vary the voltage and extend the duration of the shock in higher impedance patients.
Therefore, with a Physio-Control BTE Waveform, you might see the following waveform differences depending on patient impedance:
Philips Healthcare also uses the biphasic truncated exponential waveform in its SMART™ Biphasic device, but in this case, the voltage and current is distributed over a more narrow range of energy with the maximum current delivered at 200J, roughly equivalent to that delivered by the Physio-Control device at 360J.

The Rectilinear Biphasic Waveform (RBW) is used by ZOLL Medical, and it differs from both the BTE waveform devices. ZOLL fixes voltage at the maximum and varies resistance in order to deliver constant current across the broad range of patients. As with Philips, 200 Joules is the maximum setting on the defibrillator, however, this maximum represents more voltage on the capacitor than either Physio-Control or Philips has available.
Additionally, the duration of the ZOLL RBE waveform is fixed at 10 msec based upon work by Gliner et al.1 which indicates that the defibrillation threshold decreases with increasing time up to a point around 10-12 msec, after which it begins to increase. As there is concern in the literature about the effects of current on myocardial stunning, ZOLL chooses not to go beyond that threshold.2
The ZOLL RBW defibrillator divides impedance into two components: equipment-based impedance and patient-based impedance. Rather than adjusting the secondary variables, such as voltage and time, the ZOLL RBW adjusts the equipment-based impedance, and adds or subtracts resistors in the equipment as required to control for an essentially “constant” current during the course of the first phase.
For example, for a 200J energy setting, the ZOLL RBW charges the capacitor to the maximum voltage regardless of patient impedance. In the case of a patient with 50 ohms of impedance, the defibrillator controller adds ohms of resistance to effectively “dampen” the amount of current being delivered to the patient. For a patient with 150 ohms of impedance, no equipment-based resistors are added, and the full amount of current is delivered to the patient. In laboratory bench tests, at 200J, ZOLL delivered 27.8A peak current and 24.0A average current to a 50 ohm resistor, and 14.8A peak current and 12.5A average current to a 150 ohm resistor. At energy settings less than 200J, the difference between peak and average current is even less, typically a maximum of 1A.

The 2005 American Heart Association (AHA) Guidelines do not include a chapter on electrical therapies and refers to the 2010 AHA Guidelines, which provides the following recommendation:
Biphasic waveforms are safe and have equivalent or higher efficacy for termination of VF when compared with monophasic waveforms. In the absence of biphasic defibrillators, monophasic defibrillators are acceptable (Class IIb, LOE B). Different biphasic waveforms have not been compared in humans with regard to efficacy. Therefore, for biphasic defibrillators, providers should use the manufacturer’s recommended energy dose (120 to 200 J) (Class I, LOE B)3.
1. Gliner et al. Circulation. 1995;92:1634-45.
2. Tang et al. Journal of American College of Cardiology. 1999;34:815-822.
3. Link MS, Atkins DL, Passman RS, Halperin HR, Samson RA, White RD, Cudnik MT, Berg MD, Kudenchuk PJ, Kerber RE. Part 6: electrical therapies: automated external defibrillators, defibrillation, cardioversion, and pacing: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(suppl 3):S706–S719.